
Conversion Therapy Bans
Impact On Treating Gender Dysphoria
OUR VIEWPOINT
ReIME supports the right of young people to explore identities, including sexualities and gender. However, we believe that therapies that address same-sex sexual attraction and those intended to explore gender identities are distinct, with distinctly different evidentiary histories, concerns and outcomes. Specifically, we strongly believe that exploration of gender identities should not be stymied or prematurely foreclosed, especially when such foreclosure may lead to permanent, invasive medical procedures; and reify substandard care for a vulnerable population.
Legislation and policies that prohibit persons and entities from offering products and services that are intended to change a minor’s “gender identity” often include oblique, vague and overly broad blanket references to “efforts to change behaviors and gender expressions” without clearly defining what those services and products entail. As such, we believe they have a detrimental chilling effect that inhibit the provision of an array of services and therapies needed by this young developing population and, therefore, can present a barrier to best practices.
The issues around the treatment of “gender identity” and the treatment of same-sex romantic or sexual attraction are distinct – requiring “different models of understanding” and should not be conflated. (Bewley 2019.) While homosexuality was removed from the DSM as a mental health disorder in 1973, “gender dysphoria” is a delineated mental disorder in the current DSM-V with different attributes assigned to children and adolescents which are generally characterized by distress or problems functioning associated with the individual’s preferences related to the opposite gender or their experienced/expressed gender and their assigned gender. (APA 2013.) Consequently, offering services to eliminate or lessen gender dysphoria – a recognized disorder – is not the same as offering services to eliminate or “change” same-sex sexual attraction. And should not be treated as the same or subject to the same prohibitions.
In addition, the prohibition of offering services with respect to same-sex sexual attraction is based on numerous unequivocal studies that have shown such services that proffer to “change an individual’s sexuality” are misleading and fraudulent as they are ineffectual and create psychological trauma. (Drescher et al 2016.) By contrast, all studies ever conducted on minors, including the most recent studies demonstrate that a majority (61-88%) will resolve their dysphoria if they are not socially transitioned (i.e., provided confirming psycho/social treatment). (Waillen et al 2008; Drummond et al 2008; Signh, D. 2012; Steensma et al 2013.) And there are no studies to show that the long term well being of minors is harmed by exploratory therapies such as “watchful waiting” for prepubescent children that encourage them to explore and remain curious about their gender identity, and affirm them in this exploration without being prematurely confirmed through social transition. Watchful waiting is the prevailing standard of care in United Kingdom and Australia. Furthermore, if a gender identity is confirmed prematurely, it will not only make it difficult and distressing for the child/youth to subsequently revert or change to their original or a different gender identity or expression, it may also result in long term physical consequences – consequences not attendant to confirmation of a youth’s sexuality. Consequently, unlike same-sex sexual attraction, an evidentiary basis for the prohibition of offering services and products to children and adolescents related to gender identity and expression – does not exist. And doing so may be harmful to their long term physical well being.
Finally, minors are now presenting to gender clinics with gender dysphoria symptoms in unprecedented numbers and with complex case histories. They present at different times (prepubescent and adolescent), with differing amounts of gender dysphoria (moderate and acute), with differing neurodiverse profiles (50% of adolescents are on the ASD spectrum – See Graph), and co-morbid conditions (depression, anxiety, and personality disorders – Kaltiala-Heino et al 2015). Restricting the types of services that may be provided, including but not limited to extended assessment services because they do not affirm an individual’s gender identity – but rather seek to explore it – is limiting therapists to providing only one service, and, consequently, substandard care.
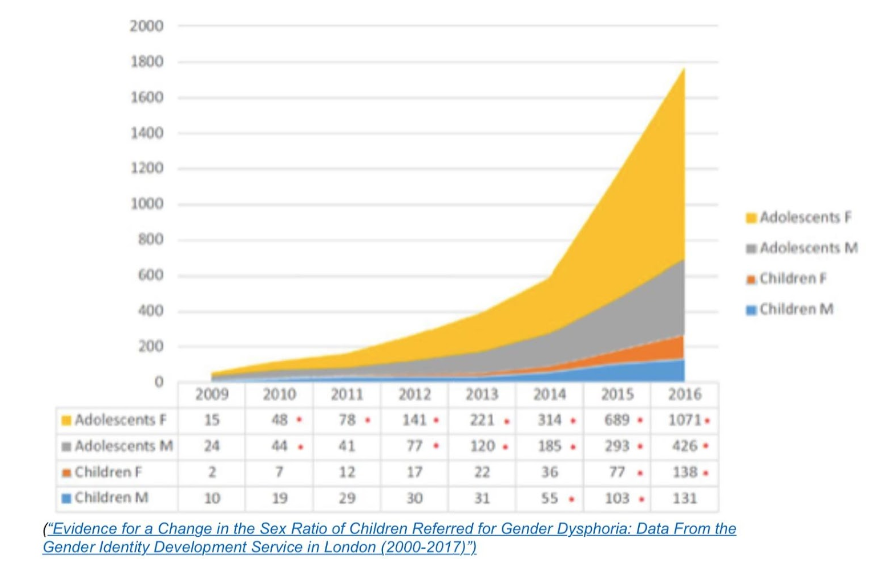
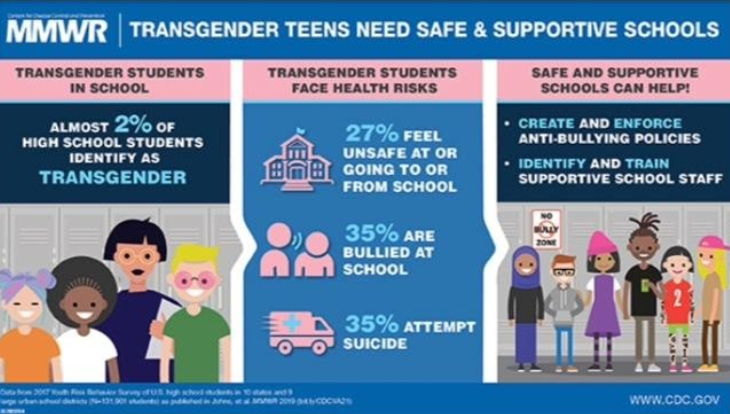
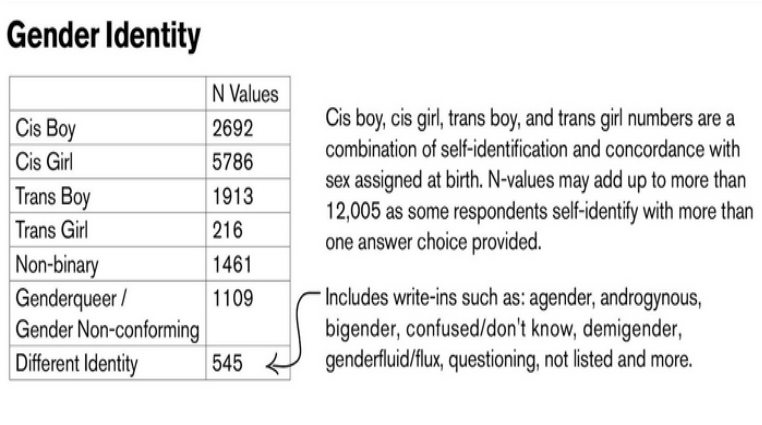
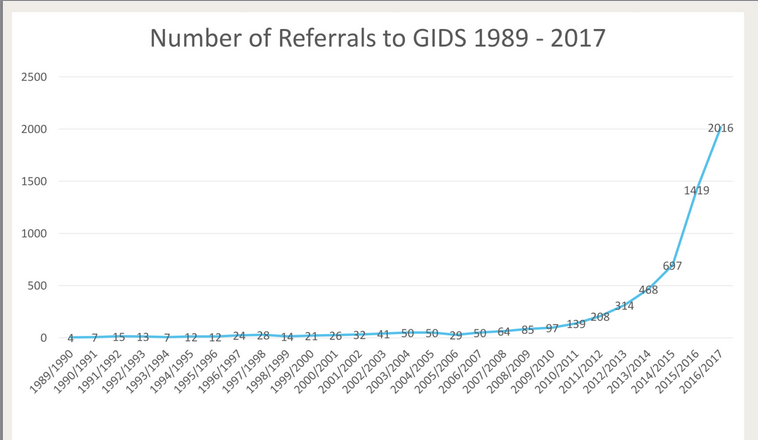
Specifically, in the last five years, gender clinics have documented a 1000% increase in youth, ages 12 -17 with no prior symptoms of gender variance. Two-thirds of this population are girls – a complete inversion of previous statistics wherein boys had outnumbered girls in the same proportions. (See attached GIDS graphs.) Similarly, the recent CDC Survey estimates that 2% of all high school students in the U.S. now identify as Transgender. (CDC Survey 2019.) While the CDC Survey does not aggregate their findings according to natal sex, The Human Rights Campaign’s LGBTQ Online Youth Survey in 2018 (with 12,000 respondents) found that LGBTQ adolescent females identify as Transgender 9:1 over adolescent boys. (See attached HRC graph.) The reasons behind this unprecedented increase in adolescent cases of gender dysphoria is unknown and is currently being studied. It is also not known whether and to what extent the gender expression of this newly presenting population is stable in comparison to those of children who present earlier and persist.
There is widespread concern that the vastly disproportionate increase in adolescent girls presenting may reflect concomitant increases in social and sexual anxiety, depression, self- harm, eating disorders and body rejection known to affect them at the onset of somatic and psycho/social changes during puberty. Adolescent-onset gender dysphoria – – particularly in natal females – – may in the long term be subject to higher rates of fluidity. For this reason, many gender clinics have adopted an “extended assessment” protocol to best treat adolescents. (Churcher Clarke 2019.) In this context, mental health professionals should be able to fully explore all issues affecting an adolescent as well as provide information regarding the possible long term risks of irreversible medical interventions without concern that offering such appropriate exploration and information could be construed as an impermissible “effort to change” the individual’s gender identity.
In conclusion, mental health professionals should have the clear latitude where appropriate to offer a therapy such as “watchful waiting” or “extended assessments” to an individual without concern for disciplinary action. Blanket bans prohibiting the offering of services and products designed to help a minor resolve their dysphoria and desist is tantamount to withholding from them the care necessary to best safeguard their long term well-being.
CITATIONS/GRAPHS
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th edn, American Psychiatric Association, Arlington.
Bewley, S. (2019). Response to Safeguarding LGBT+ adolescents: Safeguarding adolescents from premature permanent medicalization. BMJ; 364:1245.
Churcher Clarke, A., & Spoliadis, A. (2019). ‘Taking the lid off the box:’ The value of extended clinical assessment for adolescents presenting with gender identity difficulties. Clinical Child Psychology and Psychiatry, Spec. Ed., 1-15.
Drescher J, Schwartz A, Casoy, F. (2016). The Growing Regulation of Conversion Therapy. J Med Regular; 102(2): 7-12.
Drummond, K.D., Bradley, S.J., Badali-Peterson, M., & Zucker, K.J. (2008). A follow-up study of girls with gender identity disorder. Developmental Psychology, 44, 34-45.
Kaltiala – Heino, R. Summary, M., Tyolajarvi, M. & Lindbergh, N. (2015). 2 years of GI service for minors:overrepresentation of natal girls with servers problems in adolescent development. Child and Adolescent Psychiatry and Mental Health 9:9.
Singh, D. (2012). A follow-up study of boys with gender identity disorder. Unpublished doctoral dissertation, University of Toronto
Steensma, T. D., McGuire, J.K, Kreukels, B.P.C., Beckmann, A.J., & Cohen-Kettenis, P. T. (2013). Factors associated with desistance and persistence of childhood gender dysphoria: A quantitative follow-up study. Journal of American Academy of Child and Adolescent Psychiatry, 52, 582-590.
Wallien, M.S.C., & Cohen-Kettenis, P.T. (2008). Psychosexual outcome of gender-dysphoric children. Journal of American Academy of Child and Adolescent Psychiatry, 47, 1413-1423.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}